Temporomandibular joint disorder (TMJD or TMD), or TMJ syndrome, is an umbrella term covering acute or chronic inflammation of the temporomandibular joint, which connects the mandible to the skull. The disorder and resultant dysfunction can result in significant pain and impairment. Because the disorder transcends the boundaries between several health-care disciplines — in particular, dentistry, neurology, physical therapy, and psychology — there are a variety of treatment approaches.
The temporomandibular joint is susceptible to many of the conditions that affect other joints in the body, including ankylosis, arthritis, trauma, dislocations, developmental anomalies, and neoplasia.
Signs and symptoms
Signs and symptoms of temporomandibular joint disorder vary in their presentation and can be very complex. Often the symptoms will involve more than one of the numerous TMJ components: muscles, nerves, tendons, ligaments, bones, connective tissue, and the teeth. Ear pain associated with the swelling of proximal tissue is a symptom of temporomandibular joint disorder.
Muscles
TMJ diagram
Disorders of the muscles of the temporomandibular joint are the most common complaints by TMD patients. The two major observations concerning the muscles are pain and dysfunction. The dysfunction can present as trismus or limitation of jaw movement ranging from minor to severe. In milder cases, the only representation may be joint sound such as clicking or popping. These symptoms of TMD are often caused by overusage of the muscles of mastication. Common causes include chewing gum continuously, biting habits (fingernails and pencils), grinding habits, and clenching habits.
Most cases of TMJ, however, are not so simple. Deep-space infections with resulting trismus or neoplams about the joint may mimic TMJ dysfunction. Muscle pain can sometimes be associated with trigger points in muscle tissue. These trigger points can be localized by digital palpation, both intraorally and extraorally. This is known as Myofascial pain syndrome.
Any dysfunction of the muscles may cause the teeth to occlude (bite) with each other incorrectly; if teeth are traumatized by this, they may become sensitive, demonstrating one of the many interplays between muscle, joint, and tooth.
Temporomandibular joints
This is arguably the most complex set of joints in the human body. Unlike typical finger or vertebral junctions, each TMJ actually has two joints, which allow it to both rotate and to translate (slide). With use, it is common to see wear of both the bone and cartilage components of it. Clicking is common, as are popping motions and deviations in the movements of the joint. It is considered a TMJ disorder when pain is involved.
In a healthy joint, the surfaces in contact with one another (bone and cartilage) do not have any receptors to transmit the feeling of pain. The pain therefore originates from one of the surrounding soft tissues. When receptors from one of these areas are triggered, the pain causes a reflex to limit the mandible's movement. Furthermore, inflammation of the joints can cause constant pain, even without movement of the jaw.
Due to the proximity of the ear to the temporomandibular joint, TMJ pain can often be confused with ear pain. The pain may be referred in around half of all patients and experienced as otalgia (earache). Conversely, TMD is an important possible cause of secondary otalgia. Treatment of TMD may then significantly reduce symptoms of otalgia and tinnitus, as well as atypical facial pain. Despite some of these findings, some researchers question whether TMD therapy can reduce symptoms in the ear, and there is currently an ongoing debate to settle the controversy.
The dysfunction involved is most often in regards to the relationship between the condyle of the mandible and the disc. The sounds produced by this dysfunction are usually described as a "click" or a "pop" when a single sound is heard and as "crepitation" or "crepitus" when there are multiple, rough sounds
Teeth
Disorders of the teeth can contribute to TMJ dysfunction. Impaired tooth mobility and tooth loss can be caused by destruction of the supporting bone and by heavy forces being placed on teeth. The movement of the teeth affects how they contact one another when the mouth closes, and the overall relationship between the teeth, muscles, and joints can be altered. Pulpitis, inflammation of the dental pulp, is another symptom that may result from excessive surface erosion. Maybe the most important factor is the way the teeth meet together: the equilibration of forces of mastication and therefore the displacements of the condyle.
Precipitating factors
There are many external factors that place undue strain on the TMJ. These include but are not limited to the following:
Over-opening the jaw beyond its range for the individual or unusually aggressive or repetitive sliding of the jaw sideways (laterally) or forward (protrusive). These movements may also be due to parafunctional habits or a malalignment of the jaw or dentition. This may be due to:
Trauma
Repetitive unconscious jaw movements called bruxing.
Malalignment of the occlusal surfaces of the teeth due to dental defect or neglect.
Jaw thrusting (causing unusual speech and chewing habits).
Excessive gum chewing or nail biting.
Size of foods eaten.
Degenerative joint disease, such as osteoarthritis or organic degeneration of the articular surfaces, recurrent fibrous and/or bony ankylosis, developmental abnormality, or pathologic lesions within the TMJ
Myofascial pain dysfunction syndrome
Lack of Overbite
Treatment
Restoration of the occlusal surfaces of the teeth
If the occlusal surfaces of the teeth or the supporting structures have been damaged due to dental neglect, periodontal diseases or trauma, the proper occlusion should be restored.
Pain relief
While conventional analgesic pain killers such as paracetamol (acetaminophen) or NSAIDs provide initial relief for some sufferers, the pain is often more neuralgic in nature, which often does not respond well to these drugs.
An alternative approach is for pain modification, for which off-label use of low-doses of Tricyclic antidepressant that have anti-muscarinic properties (e.g. Amitriptyline or the less sedative Nortriptyline) generally prove more effective.
Long-term approach
It is suggested that before the attending dentist commences any plan or approach utilizing medications or surgery, a thorough search for inciting para-functional jaw habits must be performed. Correction of any discrepancies from normal can then be the primary goal.
An approach to eliminating para-functional habits involves the taking of a detailed history and careful physical examination. The medical history should be designed to reveal duration of illness and symptoms, previous treatment and effects, contributing medical findings, history of facial trauma, and a search for habits that may have produced or enhanced symptoms. Particular attention should be directed in identifying perverse jaw habits, such as clenching or teeth grinding, lip or cheek biting, or positioning of the lower jaw in an edge-to-edge bite. All of the above strain the muscles of mastication (chewing) and results in jaw pain. Palpation of these muscles will cause a painful response.
Treatment is oriented to eliminating oral habits, physical therapy to the masticatory muscles, and alleviating bad posture of the head and neck. A flat-plane full-coverage oral appliance, e.g. a non-repositioning stabilization splint, often is helpful to control bruxism and take stress off the temporomandibular joint, although some individuals may bite harder on it, resulting in a worsening of their conditions. The anterior splint, with contact at the front teeth only, may then prove helpful. This method of treatment is often referred to as "splint therapy."
According to the National Institute of Dental and Craniofacial Research (NIDCR) of the National Institutes of Health (NIH), TMJ treatments should be reversible whenever possible. That means that the treatment should not cause permanent changes to the jaw or teeth.Examples of reversible treatments are:
Over-the-counter pain medications, used according to manufacturers’ instructions.
Prescription medications prescribed by a healthcare provider.
Gentle jaw stretching and relaxation exercises you can do at home. Your healthcare provider can recommend exercises for your particular condition, if appropriate.
Feldenkrais TMJ Program, uses a unique understanding of human neurology to reduce chronic tension in the jaw, face, neck, and upper back, and to reverse long-standing movement habits responsible for the original TMJ symptoms.
Stabilization splint (biteplate, nightguard) is the most widely used treatment for TMJ and jaw muscle problems; however, the actual effectiveness of these splints is unclear. If an oral splint is recommended, it should be used only for a short time and should not cause permanent changes in the bite. If a splint causes or increases pain, stop using it and tell your healthcare provider. Avoid using over-the-counter mouthguards for TMJ treatment. If a splint is not properly fitted, the teeth may shift and worsen the condition.
Mandibular Repositioning Devices can be worn for a short time to help alleviate symptoms related to painful clicking when opening the mouth wide, but 24-hour wear for the long term may lead to changes in the position of the teeth that can complicate treatment. A typical long-term permanent treatment (if the device is proven to work especially well for the situation) would be to convert the device to a flat-plane bite plate fully covering either the upper or lower teeth and to be used only at night.
What may be concluded is that there are various treatment modalities which a well-trained experienced dentist may employ to relieve symptoms and improve joint function. They include:
Manual adjustment of the bite by grinding the teeth
Mandibular repositioning splints which move the jaw, ligaments and muscles into a new position and myofunctional therapy
Reconstructive dentistry
Orthodontics
Arthrocentesis (joint irrigation)
Surgical repositoning of jaws to correct congenital jaw malformations such as prognathism and retrognathia
Replacement of the jaw joint(s) or disc(s) with TMJ implants (This should be considered only as a treatment of last resort.)
Attempts in the last decade to develop surgical treatments based on MRI and CAT scans now receive less attention. These techniques are reserved for the most recalcitrant cases where other therapeutic modalities have changed. Exercise protocols, habit control, and splinting should be the first line of approach, leaving oral surgery as a last resort. Certainly a focus on other possible causes of facial pain and jaw immobility and dysfunction should be the initial consideration of the examining oral-facial pain specialist, oral surgeon or health professional. One option for oral surgery, is to manipulate the jaw under general anaesthetic and wash out the joint with a saline and anti-inflammatory solution in a procedure known as arthrocentesis. In some cases, this will reduce the inflammatory process.
A digital X-ray film revealing an impacted permanent canine. The small tooth (bottom center) is the primary canine that has not fallen out because the permanent canine has become impacted in an abnormal direction.
Impacted and embedded teeth are the two main types of unerupted teeth found in the mouth, and can sometimes be confused with each other.
An orthopantomogram revealing four impacted Wisdom teeth.
In cases of both impacted and embedded teeth, the teeth remain below the surface of the gum and sometimes bone, rather than erupting into an exposed position within the mouth; however, the reason for the failure to erupt differs. Impacted teeth result from a situation in which an unerupted tooth is wedged against another tooth or teeth or otherwise directed so that it cannot erupt normally. In contrast, an embedded tooth is an unerupted tooth that is covered, usually completely, with bone. The former is "physically" blocked in its path of eruption, while the latter is compromised by its lack of eruptive force often without known etiology. Certain systemic and local pathologic conditions may be associated with both (i.e., cleidocranial dysostosis).
Impaction classifications
There are numerous classification systems used to identify the specific manner in which a tooth is impacted. One of the most simple distinctions made is whether a tooth is impacted completely within bone or whether it has broken through the bony cortex and is partially or completely covered in gingival tissue; the former would be termed bony impaction, while the latter would be termed soft-tissue impaction, and both classifications may present as partial or complete.[1]
Mandibular third molars are the most commonly found unerupted teeth, while maxillary third molars are second most common.
Labeled photograph of alveolar osteitis ("dry socket"), one week post-operative.
In dentistry, a dry socket is a layman's term for alveolar osteitis. The alveolus is the part of the jawbone that supports the teeth, and osteitis means simply “bone inflammation”. It is an irritation of the bone open to the oral cavity after the loss of or premature disintegration of the blood clot.
Alveolar osteitis is a painful phenomenon that most commonly occurs a few days following the removal of mandibular (lower) wisdom teeth. It occurs when the blood clot within the healing tooth extraction site is disrupted. In rare cases, the removal of the upper wisdom teeth can also result in alveolar osteitis.
Signs and symptoms
As with any extraction of a tooth, some pain is to be expected, as the gums surrounding the former location will be damaged to a certain degree. This is especially so in extractions of impacted wisdom teeth, which may not have properly erupted; in these cases, the gums are cut open to allow access to the tooth, then sutured shut.
However, a dry socket typically presents as a sharp and sudden increase in pain commencing 2–5 days following the extraction of a mandibular molar, most commonly the third molar. It can also be accompanied by a foul taste or smell.
The pain, which often radiates up and down the head and neck, can be extremely unpleasant for the patient. It will often cause pain in the ears as well. A dry socket is not an infection, and is not directly associated with swelling because it occurs entirely within bone — it is a phenomenon of inflammation within the bony lining of an empty tooth socket.
Prevention
True alveolar osteitis, as opposed to simple postoperative pain, occurs in only about 5–10% of extractions (primarily of the lower molar teeth). No one knows for certain how or why dry sockets develop following dental extraction but certain factors are associated with increased risk. One of these factors is the complexity of the extraction. Smoking, which can impede healing of wounds anywhere in the body, is another possible contributing factor, possibly due to the decreased amount of oxygen available in the healing tissues. It is advisable to avoid smoking for at least 48 hours following tooth extraction to reduce the risk of developing dry socket. Additional factors increasing risk of dry socket include the use of hormonal contraception by female patients, and the amount of surgically-induced trauma to the bone required at the time of the procedure (for this reason, operator experience plays a role). Women are generally at higher risk than men of developing dry socket, because estrogen slows down healing. Dentists recommend that their female patients have extractions performed during the last week of their cycle, when estrogen levels are lowest, to minimize chances of developing dry socket.
Patients are also advised to avoid drinking through a straw as the negative pressure created by drawing liquids through the straw can dislodge the clot. Additionally, patients may be told not to spit out saliva (or anything else for that matter) excessively due to the negative pressure created in the mouth immediately prior to spitting. Maintaining good oral hygiene during the healing period by brushing all non-tender areas regularly and rinsing with warm salt water is often advised, beginning 24 hours after the extraction.
Treatment
The pain from alveolar osteitis usually lasts for 24–72 hours. There is no real treatment for dry socket — it is a self-limiting condition that will improve and disappear with time — but certain interventions can significantly decrease pain during an episode of dry socket. These interventions usually consists of a gentle rinsing of the inflamed socket followed by the direct placement with in the socket of some type of sedative dressing, which soothes the inflamed bone for a period of time and promotes tissue growth. This is usually done without anesthesia. The active ingredients in these sedative dressings usually include natural substances like zinc oxide, eugenol, and oil of cloves. It is usually necessary to have this done for two or three consecutive days, although occasionally it can take longer. Because true dry socket pain is so intense, additional analgesics are sometimes prescribed.
Tooth Interior Fatigue Fracture (TIFF) on intermediate gear
The TIFF fracture surface has a distinct plateau in the central part along the tooth width and approximately mid-height of the tooth.
Tooth Interior Fatigue Fracture, (TIFF), is a type of gear failure. The failure is characterised by a fracture at approximately mid-height on the tooth of the gear. This distinguishes it from a tooth root fatigue failure. The crack for a TIFF is initiated in the interior of the tooth. This distinguishes TIFF from other fatigue failures of gears. TIFF has been observed in case-hardened idlers (i.e. gear wheels loaded on both flanks during each revolution).
The TIFF fracture surface has a distinct plateau in the central part along the tooth width and approximately mid-height of the tooth. In a close-up of the cross-section of the TIFF small wing cracks are observed. The presence of the wing crack indicates that the main crack has propagated from the centre of the tooth toward the tooth flank.
The crack-producing stresses of TIFF are twofold: i) constant residual tensile stresses in the interior of the tooth due to case hardening; and ii) alternating stresses due to the idler usage of the gear wheel.
Contact fatigue begins with surface distress, which can grow to spalling. In severe cases a secondary crack can grow from a spalling crater through the tooth thickness and a part of the tooth can fall off. In contrast to the fracture of severe contact fatigue, spalling craters are not necessary at the flank surface for a TIFF.
A young boy after losing two baby teeth, exfoliated in response to the permanent teeth beneath, which will erupt through the gums to take their place.
Tooth loss is when one or more teeth come loose and fall out. Tooth loss is normal for deciduous teeth (baby teeth), when they are replaced by a person's adult teeth. Otherwise, losing teeth is undesirable and is the result of injury or disease, such as mouth trauma, tooth injury, tooth decay, and gum disease. The condition of being toothless or missing one or more teeth, is called edentulism.
Prevention of tooth loss
Tooth loss due to tooth decay and gum disease may be prevented by practicing good oral hygiene, and regular check-ups (twice per year) at the dentist's office.
In contact sports, risk of mouth trauma and tooth injury is reduced by wearing mouthguards and helmets with a facemask (e.g., football helmet, and goalie mask).
Missing tooth replacement
There are three basic ways to replace a missing tooth or teeth, including a fixed dental bridge, dentures, and dental implants.
Research in tooth regeneration
Researchers in Japan have successfully regrown fully functional teeth in mice. Epithelial and mesenchymal cells were extracted from the mice, cultured to produce a tooth "germ," and the germ was then implanted into the bone at the space of a missing tooth. A tooth of the correct external and internal structure, hardness, strength and sensitivity later erupted in the space, eventually meeting the opposing tooth in a manner similar to an original natural tooth. This technique may be a possible future treatment for replacement of missing teeth.
A tooth abscess or root abscess is pus enclosed in the tissues of the jaw bone at the tip of an infected tooth. Usually the abscess originates from a bacterial infection that has accumulated in the soft pulp of the tooth.
Abscesses typically originate from dead pulp tissue, usually caused by untreated tooth decay, cracked teeth or extensive periodontal disease. A failed root canal treatment may also create a similar abscess.
There are three types of dental abscess. A gingival abscess that involves only the gum tissue, without affecting either the tooth or the periodontal ligament. A periapical abscess starts in the dental pulp. A periodontal abscess begins in the supporting bone and tissue structures of the teeth.
Presentation and symptoms
"The main symptom is a severe toothache. The pain is continuous and may be described as gnawing, sharp, shooting, or throbbing." Putting pressure or warmth on the tooth may induce extreme pain. There may be a swelling present at either the base of the tooth, the gum, and/or the cheek.
A chronic abscess may be painless but still have a swelling present on the gum. It is important to get anything that presents like this checked by a dental professional as it may become acute later.
In some cases, a tooth abscess may perforate bone and start draining into the surrounding tissues creating local facial swelling. In some cases, the lymph glands in the neck will become swollen and tender in response to the infection. It may even feel like a migraine as the pain can transfer from the infected area. The pain does not normally transfer across the face, only upwards or downwards as the nerves that serve each side of the face are separate.
Treatment
In the short term, the topical application of oil of cloves, which contains Eugenol, to the infected area is well-documented as an effective remedy.
Successful treatment of a dental abscess centers on the reduction and elimination of the offending organisms. If the tooth can be restored, root canal therapy can be performed. Nonrestorable teeth must be extracted, followed by curettage of all apical soft tissue.
Unless they are symptomatic, teeth treated with root canal therapy should be evaluated at 1- and 2-years intervals to rule out possible lesional enlargement and to ensure appropriate healing.
Abscesses may fail to heal for several reasons:
Cyst formation
Inadequate root canal therapy
Vertical root fractures
Foreign material in the lesion
Associated periodontal disease
Penetration of the maxillary sinus
Following conventional, adequate root canal therapy, abscesses that do not heal or enlarge are often treated with surgery and filling the root tips; and will require a biopsy to evaluate the diagnosis.
Untreated consequences
If left untreated, a severe tooth abscess may become large enough to perforate bone and extend into the soft tissue eventually becoming osteomyelitis and cellulitis respectively. From there it follows the path of least resistance and may spread either internally or externally. The path of the infection is influenced by such things as the location of the infected tooth and the thickness of the bone, muscle and fascia attachments.
External drainage may begin as a boil which bursts allowing pus drainage from the abscess, intraorally (usually through the gum) or extra orally. Chronic drainage will allow an epithelial lining to form in this communication to form a pus draining canal (fistula). Sometimes this type of drainage will immediately relieve some of the painful symptoms associated with the pressure.
Internal drainage is of more concern as growing infection makes space within the tissues surrounding the infection. Severe complications requiring immediate hospitalisation include Ludwig's angina, which is a combination of growing infection and cellulitis which closes the airway space causing suffocation in extreme cases. Also infection can spread down the tissue spaces to the mediastinum which has significant consequences on the vital organs such as the heart. Another complication, usually from upper teeth, is a risk of septicaemia (infection of the blood), from connecting into blood vessels, brain abscess, (extremely rare) or meningitis, (also rare).
Depending on the severity of the infection, the sufferer may feel only mildly ill, or may in extreme cases require hospital care.
A profile of a smile, exhibiting significant wear, especially on the maxillary incisors. Even though the teeth are in an edge-to-edge position, the teeth are in maximum intercuspation; this patient possesses a Class III occlusion.
Bruxism (from the Greek βρυγμός (brugmós), "gnashing of teeth") is characterized by the grinding of the teeth and is typically accompanied by the clenching of the jaw. It is an oral parafunctional activity that occurs in most humans at some time in their lives. In most people, bruxism is mild enough not to be a health problem. While bruxism may be a diurnal or nocturnal activity, it is bruxism during sleep that causes the majority of health issues and can even occur during short naps. Bruxism is one of the most common sleep disorders.
Etiology
Numerous articles have incorrectly cited bruxism as being a reflex chewing activity, but bruxism is more accurately classified as a habit. Reflex activities happen reliably in response to a stimulus, without involvement of subconscious brain activity, and bruxism does not. All habitual activities are triggered by one kind of stimulus or another, and that does not make the habit a reflex. Chewing is a complex neuromuscular activity that is controlled by subconscious processes, with higher control by the brain. During sleep, the subconscious processes become active, while the higher control is inactive, resulting in bruxism. Some bruxism activity is rhythmic (like chewing), and some is sustained (clenching). Researchers classify bruxism as "a habitual behavior, and a sleep disorder."
The etiology of problematic bruxism is unknown, though several conditions are known to be linked to bruxism. It is theorized that certain medical conditions can trigger bruxism, including digestive ailments and anxiety.
Signs
The effects of bruxism on an anterior tooth, revealing the dentin and pulp which are normally hidden by enamel
Most bruxers are not aware of their bruxism, and only 5% go on to develop symptoms, such as jaw pain and headaches, which will require treatment. In many cases, a sleeping partner or parent will notice the bruxism before the person experiencing the problem becomes aware of it.
Bruxism can result in abnormal wear patterns of the occlusal surface, abfractions and fractures in the teeth. This type of damage is categorised as a sign of occlusal trauma.
Over time, dental damage will usually occur. Bruxism is the leading cause of occlusal trauma and a significant cause of tooth loss and gum recession.
In a typical case, the canines and incisors of the opposing arches are moved against each other laterally, i.e., with a side-to-side action, by the medial pterygoid muscles that lie medial to the temporomandibular joints bilaterally. This movement abrades tooth structure and can lead to the wearing down of the incisal edges of the teeth. People with bruxism may also grind their posterior teeth, which will wear down the cusps of the occlusal surface. Bruxism can be loud enough to wake a sleeping partner. Some individuals will clench the jaw without significant lateral movements. Teeth hollowed by previous decay (caries), or dental drilling, may collapse, as the cyclic pressure exerted by bruxism is extremely taxing on the tooth structure.
Symptoms
Patients may present with a variety of symptoms, including:
Morning migraines
Morning headaches
Jaw pain
TMJ pain
Facial muscle and nerve pain
Earache
Sinus pain
Tinnitus (ringing in the ear)
Vertigo
Neck pain
Shoulder pain
Back pain
Poor sleep
Waking exhausted
Stress or tension
Depression
Eating disorders
Insomnia
Daytime sleepiness
Eye irritation
Head tingling
Sequelae
Eventually, bruxism shortens and blunts the teeth being ground and may lead to myofacial muscle pain, temporomandibular joint dysfunction and headaches. In severe, chronic cases, it can lead to arthritis of the temporomandibular joints. The jaw clenching that often accompanies bruxism can be an unconscious neuromuscular daytime activity, which should be treated as well, usually through physical therapy (recognition and stress response reduction).
Diagnoses
Bruxism can sometimes be difficult to diagnose by visual evidence alone, as it is not the only cause of tooth wear. Over-vigorous brushing, abrasives in toothpaste, acidic soft drinks and abrasive foods can also be contributing factors, although each causes characteristic wear patterns that a trained professional can identify. Additionally, the presenting symptoms may be difficult for a physician to attribute to bruxism.
The effects of bruxism may be quite advanced before sufferers are aware they brux. Abraded teeth are usually brought to the patient's attention during a routine dental examination. If enough enamel has been abraded, the softer dentin will be exposed, and abrasion will accelerate. This opens the possibility of dental decay and tooth fracture, and in some people, gum recession. Early intervention by a dentist is advisable.
The most reliable way to diagnose bruxism is through EMG (electromyographic) measurements. These measurements pick up electrical signals from the chewing muscles (masseter and temporalis). This is the method used in sleep labs. There are three forms of EMG measurement available to consumers for use outside sleep labs. The first is bedside EMG units similar to those used by sleep labs. These units can be purchased for about $2000 and pick up their signals from facial muscles through wires connecting the bedside unit to electrodes that are adhesively attached to the user's face. TENS electrodes or ECG electrodes may be used.
The second type of EMG measurement available to consumers is a self-contained EMG measurement headband sold under the trade name SleepGuard, available on loan from some dentists or at a rental rate of $50 per month from the manufacturer. The EMG measurement headband does not require adhesive electrodes or wires attached to the face. While it does not record the exact time, duration, and strength of each clenching incident as the most expensive bedside EMG monitors do, it does record the total number of clenching incidents and the total clenching time each night. These two numbers easily distinguish clenching from rhythmic grinding and allow dentists to quantify severity levels accurately.
Bedside EMG units and the self-contained EMG measurement headband can both be used either in silent mode as a diagnosis measurement or in biofeedback mode as a treatment.
A third method of diagnosis using EMG is available in disposable form under the trade name BiteStrip. The BiteStrip is a self-contained EMG module that adhesively mounts to the side of the face over the masseter muscle. The BiteStrip can only do one night of measurement and does not display the clench count or total clenching time, but rather provides a single-digit display related to bruxism severity. The BiteStrip provides significantly less information than an EMG bedside unit or EMG headband and costs about $60 per day to use.
Associated factors
The following factors are associated with bruxism.
Disturbed sleep patterns and other sleep disorders (obstructive sleep apnea, hypopnea, snoring, moderate daytime sleepiness)
Malocclusion, in which the upper and lower teeth occlude in a disharmonic way, e.g., through premature contact of back teeth[citation needed]
Relatively high levels of consumption of caffeinated drinks and foods, such as coffee, colas, and chocolate
High levels of blood alcohol
Smoking
High levels of anxiety, stress, work-related stress, irregular work shifts, stressful profession and ineffective coping strategies
Drug use, such as SSRIs and stimulants, including methylenedioxymethamphetamine (ecstasy), methylenedioxyamphetamine (MDA), methylphenidate and other amphetamines, including those taken for medical reasons
Hypersensitivity of the dopamine receptors in the brain
GHB and similar GABA-inducing analogues such as Phenibut, when taken with high frequency
Disorders such as Huntington's and Parkinson's diseases
Obsessive Compulsive Disorder
Chemical drugs
Treatment
There is no single accepted cure for bruxism. However, treatments are available.
Bruxism may be reduced or even eliminated when the associated factors, e.g., sleep disorders, are treated successfully.
Mouthguards and splints
Ongoing management of bruxism is based on minimizing the abrasion of tooth surfaces by the wearing of an acrylic dental guard, or splint, designed to the shape of an individual's upper or lower teeth from a bite mould. Mouthguards are obtained through visits to a dentist for measuring, fitting, and ongoing supervision. There are four possible goals of this treatment: constraint of the bruxing pattern such that serious damage to the temporomandibular joints is prevented, stabilization of the occlusion by minimizing the gradual changes to the positions of the teeth that typically occur with bruxism, prevention of tooth damage, and the enabling of a bruxism practitioner to judge—in broad terms—the extent and patterns of bruxism through examination of the physical indentations on the surface of the splint. A dental guard is typically worn on a long-term basis during every night's sleep. Although mouthguards are a first response to bruxism, they do not in fact help cure it. An otc soft mouthguard is not considered effective by most. These mouthguards can cost anywhere from $200 to $400.
Professional treatment is medically recommended to ensure proper fit, make ongoing adjustments as needed, and check that the occlusion (bite) has remained stable. Monitoring of the mouthguard is suggested at each dental visit.
Another type of device sometimes given to a bruxer is a repositioning splint. A repositioning splint may look similar to a traditional night guard, but is designed to change the occlusion, or bite, of the patient. Randomly controlled trials with these type devices generally show no benefit over more conservative therapies, and they should be avoided under most, if not all, circumstances.
The NTI-tss device is another option that can be considered. The NTI covers only the front teeth and prevents the rear molars from coming into contact, thus limiting the contraction of the temporalis muscle. The NTI must be fitted by one's dentist.
The efficacy of such devices is debated. Some writers propose that irreversible complications can result from the long-term use of mouthguards and repositioning splints.
Biofeedback
Various biofeedback devices are currently available, and effectiveness varies significantly depending on whether the biofeedback is used only during waking hours, or during sleep as well. Many authorities remain unconvinced of the efficacy of daytime-only biofeedback. The efficacy of biofeedback delivered during sleep can depend strongly on daytime training, which is used to establish a Pavlovian response to the biofeedback signal that persists during sleep.
The first wearable nighttime bruxism biofeedback device (a biofeedback headband introduced in 2001) was originally sold under the trademark GrindAlert by BruxCare and is now sold under the GrindAlert and SleepGuard trademarks by Holistic Technologies, which holds an exclusive worldwide license to the technology. The biofeedback headband is a battery-powered device that sounds a tone against the forehead when it senses EMG (electromyographic) muscle activity in the temporalis muscles. This device records and displays nightly data on the number of bruxism events that last for at least two seconds and the total accumulated duration of those events. The volume of the alarm and the bite force required to trigger the device are adjustable. After proper Pavlovian training during waking hours, more than 25% of users achieve significantly reduced bruxism. The biofeedback sound on the headband is designed to come on slowly, allowing users to subconsciously respond in their sleep without waking up. The manufacturer offers a free three-week trial so that only people who find the device works well for them have to pay for it and claims that less than 15% of trial units are returned.
A mild electric shock bio-feedback device for treating Bruxism, GrindCare, has been approved by the European regulatory authorities and was introduced to the market in 2008. The GrindCare device infringes the US patents on the SleepGuard/GrindAlert device, so the GrindCare device is not legal to import into the United States without a license from Holistic Technologies. The device works by using simple electrodes mounted on the skin close to the cheek bones prior to sleeping; it detects the initial muscular contractions and immediately provides insignificant pulses to the facial muscles, whereby the contractions are stopped. The device is worn on the head and reportedly reduces grinding without interfering with the sleep of the patient as described by Jadidi, Castrillon & Svensson. Thereby, facial tension, joint defects and teeth disruption are reportedly reduced.
A taste-based biofeedback method was developed by Moti Nissani, Ph.D. and is called "The Taste-Based Approach to the Prevention of Teeth Clenching and Grinding". The therapy involves suspending sealed packets containing a bad-tasting substance (e.g. hot sauce, vinegar, denatonium benzoate, etc.) between the rear molars using an orthodontic-style appliance. Any attempt to bring the teeth together will rupture the packets and alert the user to the habit. This approach finds favor with some people who prefer to relate to biofeedback as "aversive therapy". The Taste-Based Approach claims to suffer less from desensitization over time than sound-based biofeedback approaches may have, but may interrupt sleep more. (There is effectively no limit to the aversive taste of certain substances. We can therefore be sure that some harmless substance exists that will alert anyone to the habit.)
One bruxism biofeedback device which was briefly on the market but is no longer available was sold under the trademark Oralsensor. This device consisted of a pneumatic pouch embedded in a soft polymer plate that fits over upper or lower teeth. When the teeth came together with a force that exceeded a set threshold, an alarm is sounded in an earpiece worn by the user; the device is no longer sold.
In 2005, a new type of occlusive device was patented that produces a movement incompatible with teeth clenching. When nighttime bruxism occurs, people breathe through the nose. The device forces people to breathe through the mouth; by forcing the opening of the mouth, the device is claimed to stop clenching. The occlusive device has an electromyogram system that monitors the electric activity of the jaw muscle via wireless electrodes. These electrodes transfer jaw-muscle activity by radio frequency to an external monitoring system. Once the signal has been interpreted by the monitoring system, if a person clenches, the monitoring unit sends a radio frequency signal to a transceiver integrated in a mechanical actuator. The mechanical actuator has two occlusive flaps that block the nostrils, forcing breathing to occur through the mouth. Once the patient stops clenching, the flaps open, allowing breathing through the nose again. The occlusive device does not wake up people since it blocks nostrils slowly, and it never closes them completely to avoid sleep disruption.
Botox
Botulinum toxin (Botox) can be successful in lessening effects of bruxism, though serious side-effects are possible. Less than one microgram ingested or inhaled is sufficient to kill an adult human. In extremely dilute form (Botox), this toxin is used as an injectable medication that weakens (partially paralyzes) muscles and has been used extensively in cosmetic procedures to relax the muscles of the face and decrease the appearance of wrinkles. In April, 2008, a study was published in the Journal of Neuroscience that showed that facially injected Botox can and does propagate into the brains of some test animals, and the U.S. Food and Drug Administration (FDA) announced that it was beginning a safety review of Botox and other similar drugs.
Botox was not originally developed for cosmetic use. It was, and continues to be, used to treat diseases of muscle spasticity such as blepharospasm (eyelid spasm), strabismus (crossed eyes) and torticollis (wry neck). Bruxism can also be regarded as a disorder of repetitive, unconscious contraction of the masseter muscle (the large muscle that moves the jaw). In the treatment of bruxism, Botox works to weaken the muscle enough to reduce the effects of grinding and clenching, but not so much as to prevent proper use of the muscle. The strength of Botox is that the medication goes into the muscle and is not supposed to get absorbed into the body (though the new research shows it does). The procedure involves about five or six simple, relatively painless injections into the masseter muscle. It takes a few minutes per side, and the patient starts feeling the effects the next day. Occasionally, some bruising can occur, but this is quite rare. Injections must be repeated more than once per year, and the risk factor of spread of the botulinum toxin is compounded by this repetition.
The symptoms that can be helped by this procedure include:
Grinding and clenching
Morning jaw soreness
TMJ pain
Muscle tension throughout the day
Migraines triggered by clenching
Neck pain and stiffness triggered by clenching
The optimal dose of Botox must be determined for each person as some people have stronger muscles that need more Botox. This is done over a few touch-up visits with the physician injector. This treatment is expensive, but sometimes Botox treatment of bruxism can be billed to medical insurance. The effects last for about three months. The muscles do atrophy, however, so after a few rounds of treatment, it is usually possible either to decrease the dose or increase the interval between treatments.
Other authorities caution that Botox should only be used for temporary relief for severe cases and should be followed by diagnosis and treatment to prevent future bruxism or jaw clenching, suggesting that prolonged use of Botox can lead to permanent damage to the jaw muscle.
Dietary supplements
There is anecdotal evidence that suggests taking certain combinations of dietary supplements may alleviate bruxism; pantothenic acid, magnesium, and calcium are mentioned on dietary supplement websites. Calcium is known to be a treatment for gastric problems, and gastric problems such as acid reflux are known to increase bruxism.
Repairing damage
Damaged teeth can be repaired by replacing the worn natural crown of the tooth with prosthetic crowns. Materials used to make crowns vary; some are less prone to breaking than others and can last longer. Porcelain fused to metal crowns may be used in the anterior (front) of the mouth; in the posterior, full gold crowns are preferred. All-porcelain crowns are now becoming more and more common and work well for both anterior and posterior restorations. To protect the new crowns and dental implants, an occlusal guard should be fabricated to wear during sleep.
Third molar teeth (commonly referred to as wisdom teeth) consist of the mandibular and maxillary third molars; they usually appear between the ages of 17 and 25. They are called wisdom teeth because usually they come in when a person is between age 17 and 25 or older—old enough to have supposedly gained some wisdom. Most adults have four wisdom teeth, but it is possible to have more or fewer. Absence of one or more wisdom teeth is an example of hypodontia. Any extra teeth are referred to as supernumerary teeth. Wisdom teeth commonly affect other teeth as they develop - becoming impacted or "coming in sideways." They are often extracted when this occurs.
Etymology of "wisdom teeth"
They are generally thought to be called wisdom teeth because they appear so late—much later than the other teeth, at an age where people are presumably wiser than as a child, when the other teeth erupt. The English wisdom tooth is derived from Latin dens sapientiae. The same root is shared by numerous other languages. There exists a Dutch folk etymology which states that the Dutch word for wisdom tooth verstandskies is derived from "far-standing" (ver-staand) molar, and that mistranslations of the Dutch word (in which verstand translates to wisdom) are the root for corresponding words in other European languages.
Impaction
The upper left (picture right) and upper right (picture left) wisdom tooth are distoangularly impacted. The lower left wisdom tooth is horizontally impacted. The lower right wisdom tooth is vertically impacted (unidentifiable in orthopantomogram).
Impacted wisdom teeth fall into one of several categories. Mesioangular impaction is the most common form (44%), and means the tooth is angled forward, towards the front of the mouth. Vertical impaction (38%) occurs when the formed tooth does not erupt fully through the gum line. Distoangular impaction (6%) means the tooth is angled backward, towards the rear of the mouth. And finally, Horizontal impaction (3%) is the least common form, which occurs when the tooth is angled fully ninety degrees forward, growing into the roots of the second molar.
Typically distoangular impactions are the easiest to extract in the maxilla and most difficult to extract in the mandible, while mesioangular impactions are the most difficult to extract in the maxilla and easiest to extract in the mandible. Frequently, a fully erupted upper wisdom tooth requires bone removal if the tooth does not yield easily to forceps or elevators. Failure to remove distal or buccal bone while removing one of these teeth can cause the entire maxillary tuberosity to be fractured off and thereby the tearing out the floor of the maxillary sinus.
Impacted wisdom teeth may also be categorized on whether they are still completely encased in the jawbone. If it is completely encased in the jawbone, it is a bony impaction. If the wisdom tooth has erupted out of the jawbone but not through the gumline, it is called a soft tissue impaction. Sometimes the wisdom tooth fails to erupt completely through the gum bed and the gum at the back of the wisdom tooth extends over the biting surface, forming a soft tissue flap or lid around the tooth called an operculum. Teeth covered by an operculum can be difficult to clean with a toothbrush. Additional cleaning techniques can include using a needle-less plastic syringe to vigorously wash the tooth with moderately pressured water or to softly wash it with hydrogen peroxide.
However, debris and bacteria can easily accumulate under an operculum, which may cause pericoronitis, a common infection problem in young adults with partial impactions that is often exacerbated by occlusion with opposing 3rd or 2nd molars. Common symptoms include a swelling and redness of the gum around the eruption site, difficulty in opening the mouth, a bad odor or taste in the mouth, and pain in the general area which may also run down the entire lower jaw or possibly the neck. Untreated pericoronitis can progress to a much more severe infection.
If the operculum does not disappear, recommended treatment is extraction of the wisdom tooth. An alternative treatment involving removal of the operculum, called operculectomy, has been advocated. There is a high risk of permanent or temporary numbness of the tongue due to damage of the nerve with this treatment and it is no longer recommended as a standard treatment in oral surgery.
The oldest known impacted wisdom tooth belonged to a European woman of the Magdalenian period (18,000 - 10,000 BP)
Extraction
A wisdom tooth protrudes outwards from the gumline at the back of the lower teeth.
A dental officer and his assistant remove the mandibular third molar of a patient.
An extracted mandibular third molar that was horizontally impacted.
An upper and lower right wisdom tooth extracted during the same session
under local anaesthetics.
Wisdom teeth are extracted for two general reasons: either the wisdom teeth have already become impacted, or the wisdom teeth could potentially become problematic if not extracted. Potential problems caused by the presence of properly grown-in wisdom teeth include infections caused by food particles easily trapped in the jaw area behind the wisdom teeth where regular brushing and flossing is difficult and ineffective. Such infections may be frequent, and cause considerable pain and medical danger. Other reasons wisdom teeth are removed include misalignment which rubs up against the tongue or cheek causing pain, potential crowding or malocclusion of the remaining teeth (a result of there being not enough room on the jaw/ in the mouth),as well as orthodontics.
A panoramic x-ray (aka "panorex") is the best x-ray to view wisdom teeth and diagnose problems.
Post-extraction problems
There are several problems that might occur after the extraction(s) have been completed. Some of these problems are unavoidable and natural, while others are under the control of the patient. The suggestions contained in the sections below are general guidelines that a patient will be expected to abide by, but the patient should follow all directions that are given by the surgeon in addition to the following guidelines. Above all, the patient must not disregard the given instructions; doing so is extremely dangerous and could result in any number of problems ranging in severity from being merely inconvenient (dry socket) to potentially life-threatening (serious infection of the extraction sites).
Cyst around right lower wisdom tooth.
Bleeding and oozing
Bleeding and oozing is inevitable and should be expected to last up to three days (although by day three it should be less noticeable). Rinsing the mouth during this period is counter-productive, as the bleeding stops when the blood forms clots at the extraction sites, and rinsing out the mouth will most likely dislodge the clots. The end result will be a delay in healing time and a prolonged period of bleeding. However, after about 24 hours post-surgery, it is best to rinse with lukewarm saltwater to promote healing. This should be done twice a day until the swelling goes down and every 4–6 hours after that for at least a week. Gauze pads should be placed at the extraction sites, and then should be bitten down on with firm and even pressure. This will help to stop the bleeding, but should not be overdone as it is possible to irritate the extraction sites and prolong the bleeding or remove the clot. The bleeding should decrease gradually and noticeably upon changing the gauze. If the bleeding lasts for more than a day without decreasing despite having followed the surgeon's directions, the surgeon should be contacted as soon as possible. This is not supposed to happen under normal circumstances and signals that a serious problem is present. A wet tea bag can replace the gauze pads.Tannic acid contained in tea can help reduce the bleeding.
Due to the blood clots that form in the exposed sockets as well as the abundant bacterial flora in the mouth, an offensive smell may be noticeable a short time after surgery. The persistent odor often is accompanied by an equally rancid-tasting fluid seeping from the wounds. These symptoms will diminish over an indefinite amount of time, although one to two weeks is normal. While not a cause for great concern, a post-operative appointment with one's surgeon seven to ten days after surgery is highly recommended to make sure that the healing process has no complications and that the wounds are relatively clean. If infection does enter the socket, a qualified dental professional can gently plunge a plastic syringe (without the hypodermic needle) full of a mixture of equal parts hydrogen peroxide and water or chlorohexidine gluconate which also comes in the form of a mouth wash into the sockets to remove any food or bacteria that may collect in the back of the mouth. This is less likely if the person has his/her wisdom teeth removed at an early age.
Dry socket
A dry socket is not an infection; it is the event where the blood clots at an extraction site are dislodged, fall out prematurely, or fail to form. It is still not known how they form or why they form. In some cases, this is beyond the control of the patient. However, in other cases this happens because the patient has disregarded the instructions given by the surgeon. Smoking, blowing one's nose, spitting, or drinking with a straw in disregard to the surgeon's instructions can cause this, along with other activities that change the pressure inside of the mouth, such as sneezing or playing a musical instrument. The risk of developing a dry socket is greater in smokers, if the patient has had a previous dry socket, in the lower jaw, and following complicated extractions. The extraction site will become irritated and painful, due to inflammation of the bone lining the tooth socket (osteitis). The symptoms are made worse when food debris is trapped in the tooth socket. The patient should contact their surgeon if they suspect that they have a case of dry socket. The surgeon may elect to clean the socket under local anesthetic to cause another blood clot to form or prescribe medication in topical form (e.g. Alvogel) to apply to the affected site. A non-steroidal anti-inflammatory drug (NSAID) such as ibuprofen may be prescribed by the surgeon for pain relief. Generally dry sockets are self limiting and heal in a couple of weeks without treatment.
Swelling
Swelling should not be confused with dry socket, although painful swelling should be expected and is a sign that the healing process is progressing normally. There is no general duration for this problem; the severity and duration of the swelling vary from case to case. The instructions the surgeon will tell the patient for how long they should expect swelling to last, including when to expect the swelling to peak and when the swelling will start to subside. If the swelling does not begin to subside when it is supposed to, the patient should contact his or her surgeon immediately. While the swelling will generally not disappear completely for several days after it peaks, swelling that does not begin to subside or gets worse may be an indication of infection. Swelling that re-appears after a few weeks is an indication of infection caused by a bone or tooth fragment still in the wound and should be treated immediately.
Nerve injury
Mandibular division of trigeminal nerve, seen from the middle line.
This is primarily an issue with extraction of third molars, but can occur with the extraction of any tooth should the nerve be in close proximity to the surgical site. Two nerves are typically of concern and are found in duplicate (on the left and right side):
The inferior alveolar nerve, which enters the mandible at the mandibular foramen and exits the mandible at the sides of the chin from the mental foramen. This nerve supplies sensation to the lower teeth on the right or left half of the dental arch, as well as sense of touch to the right or left half of the chin and lower lip.
The lingual nerve, which branches off the mandibular branches of the trigeminal nerve and courses just inside the jaw bone, entering the tongue and supplying sense of touch and taste to the right and left half of the anterior 2/3 of the tongue as well as the lingual gingiva (i.e. the gums on the inside surface of the dental arch).
Such injuries can occur while lifting teeth (typically the inferior alveolar) but are most commonly caused by inadvertent damage with a surgical drill. Such injuries are rare and are usually temporary. Depending on the type of injury (i.e. Seddon classification: neuropraxia, axonotmesis, and neurotmesis) they can be prolonged or permanent.
Treatment controversy
Preventive removal of the third molars is a common practice in developed countries despite the lack of scientific data to support this practice. In 2006, the Cochrane Collaboration published a systematic review of randomized controlled trials in order to evaluate the effect of preventive removal of asymptomatic wisdom teeth. The authors found no evidence to either support or refute this practice. There was reliable evidence showing that preventative removal did not reduce or prevent late incisor crowding. The authors of the review suggested that the number of surgical procedures could be reduced by 60% or more. This study, however, was published in the Journal of Phytology and is not accredited by many peer review organizations.
Likewise, ClinicalEvidence published a summary, largely based on the Cochrane review, that concluded prophylactic extraction is "likely to be ineffective or harmful." The website offered the following details:
While it is clear that symptomatic impacted wisdom teeth should be surgically removed, it appears that extracting asymptomatic, disease-free wisdom teeth is not advisable due to the risk of damage to the inferior alveolar nerve.
Some non-RCT evidence suggests that the extraction of the asymptomatic tooth may be beneficial if caries are present in the adjacent second molar, or if periodontal pockets are present distal to the second molar.
Studies showed that dentists graduated from different countries or even from different dental schools in one country, may have different clinical decisions regarding third molar removal for the same clinical condition. For example, dentists graduated from Israeli dental schools may recommend more often for the removal of asymptomatic impacted third molar than dentists graduated from Latin-American or Eastern European dental schools.
In the U.K., the National Institute for Health and Clinical Excellence (an authority which appraises the cost-effectiveness of treatments for the National Health Service) has recommended that impacted wisdom teeth that are free from disease should not be operated on. Conversely, in the U.S., the American Association of Oral and Maxillofacial Surgeons (the professional organization representing oral and maxillofacial surgeons in the United States) recommends that all wisdom teeth should be removed at an early age as a prophylactic measure. This would suggest that recommendations regarding the removal of third molars vary widely from country to country, depending on the stakeholders involved.
Vestigiality and variation
Wisdom teeth are vestigial third molars that human ancestors used to help in grinding down plant tissue. The common postulation is that the skulls of human ancestors had larger jaws with more teeth, which were possibly used to help chew down foliage to compensate for a lack of ability to efficiently digest the cellulose that makes up a plant cell wall. As human diets changed, smaller jaws gradually evolved, yet the third molars, or "wisdom teeth", still commonly develop in human mouths.
Other findings suggest that a given culture's diet is a larger factor than genetics in the development of jaw size during human development (and, consequently, the space available for wisdom teeth).
Different human populations differ greatly in the percentage of the population which form wisdom teeth. Agenesis of wisdom teeth ranges from 0.2% in Bantu speakers to nearly 100% in indigenous Mexicans. The difference is related to the PAX9 gene (and perhaps other genes).
Potential uses for extracted teeth
In August 2008, it was revealed that scientists in Japan were able to successfully harvest stem cells from wisdom teeth. This discovery is of great clinical importance, as wisdom tooth extractions are a relatively common type of oral surgery. Patients who have their wisdom teeth removed are currently able to opt to have stem cells from those teeth isolated and saved, in case they should ever need the cells.
Onychophagia or nail biting is a common oral compulsive habit in children and adults, affecting around 30% of children between 7 to 10 years and 45% of teenagers.
Negative effects
Bitten fingertips can become very sensitive to pain, usually at the place the skin meets the edge of the nail. Hangnails are broken skin on the cuticle. When they are improperly removed, they are susceptible to microbial and viral infections producing whitlows. Saliva may then redden and infect the skin. Finally it may also result in the transportation of bacteria that are buried under the surface of the nail, or pinworms from anus region to mouth. Nail biting is also related to dental problems, such as gingival injury.
Regarding social effects the aesthetic aspect of the nail may affect employability, self-esteem, and interaction with other people.
Treatment
Behavioral treatments are based in discouraging the habit and replace it with a more constructive habit. The most common treatment, as it is cheap and widely available, is a special clear nail polish that has to be applied to the nails. It releases a bitter flavor on contact with the mouth which discourages the habit and has demonstrated its effectiveness. There are also mouthpieces that prevent biting.
Behavioral therapy is beneficial when simpler measures are not effective. Habit Reversal Training (HRT), seeks to "unlearn" the habit of nail biting and possibly replace it with a more constructive habit and has shown its effectiveness versus placebo both in children and adults. In addition to HRT, stimulus control therapy is used to both identify and then eliminate the stimulus that frequently triggers biting urges.
Finally nail cosmetics can help to ameliorate nail biting social effects.
Related disorders
Some related body-focused repetitive behaviors are dermatillomania (skin picking), dermatophagia (skin biting) or trichotillomania (urge to pull out hair).
A toothache, also known as odontalgia or, less frequently, as odontalgy, is an aching pain in or around a tooth. In most cases toothaches are caused by problems in the tooth or jaw, such as cavities, gum disease, the emergence of wisdom teeth, a cracked tooth, infected dental pulp (necessitating root canal treatment or extraction of the tooth), jaw disease, or exposed tooth root. Causes of a toothache may also be a symptom of diseases of the heart, such as angina or a myocardial infarction, due to referred pain. After having one or more teeth extracted a condition known as dry socket can develop, leading to extreme pain. The severity of a toothache can range from a mild discomfort to excruciating pain, which can be experienced either chronically or sporadically. This pain can often be aggravated somewhat by chewing or by hot or cold temperature. An oral examination complete with X-rays can help discover the cause. Severe pain may be considered a dental emergency. A special condition is barodontalgia, a dental pain evoked upon changes in barometric pressure, in otherwise asymptomatic but diseased teeth. Atypical odontalgia is a form of toothache present in apparently normal teeth. The pain, generally dull, often moves from one tooth to another for a period of 4 months to several years. This is most commonly reported by middle-aged women. The cause of atypical odontalgia is not yet clear.
Toothaches are sometimes caused by an irritation of the pulp, known as pulpitis. This can be either reversible or irreversible. Irreversible pulpitis can be identified by sensitivity and pain lasting longer than fifteen seconds, although an exception to this may exist if the tooth has been recently operated on. Teeth affected by irreversible pulpitis will need either a root canal or an extraction.
Destruction of a tooth by cervical decay from dental caries. This type of decay is also known as root decay.
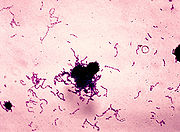
Dental caries, also known as tooth decay or cavity, is a disease wherein bacterial processes damage hard tooth structure (enamel, dentin and cementum). These tissues progressively break down, producing dental cavities (holes in the teeth). Two groups of bacteria are responsible for initiating caries: Streptococcus mutans and Lactobacilli. If left untreated, the disease can lead to pain, tooth loss, infection, and, in severe cases, death. Today, caries remains one of the most common diseases throughout the world. Cariology is the study of dental caries.
The presentation of caries is highly variable; however, the risk factors and stages of development are similar. Initially, it may appear as a small chalky area that may eventually develop into a large cavitation. Sometimes caries may be directly visible, however other methods of detection such as radiographs are used for less visible areas of teeth and to judge the extent of destruction.
Tooth decay is caused by specific types of acid-producing bacteria that cause damage in the presence of fermentable carbohydrates such as sucrose, fructose, and glucose. The mineral content of teeth is sensitive to increases in acidity from the production of lactic acid. Specifically, a tooth (which is primarily mineral in content) is in a constant state of back-and-forth demineralization and remineralization between the tooth and surrounding saliva. When the pH at the surface of the tooth drops below 5.5, demineralization proceeds faster than remineralization (i.e. there is a net loss of mineral structure on the tooth's surface). This results in the ensuing decay. Depending on the extent of tooth destruction, various treatments can be used to restore teeth to proper form, function, and aesthetics, but there is no known method to regenerate large amounts of tooth structure. Instead, dental health organizations advocate preventive and prophylactic measures, such as regular oral hygiene and dietary modifications, to avoid dental caries.
Classification
Caries can be classified by location, etiology, rate of progression, and affected hard tissues. These classification can be used to characterize a particular case of tooth decay in order to more accurately represent the condition to others and also indicate the severity of tooth destruction.
GV Black Classification of Restorations
Location
Generally, there are two types of caries when separated by location: caries found on smooth surfaces and caries found in pits and fissures. The location, development, and progression of smooth-surface caries differ from those of pit and fissure caries. G.V. Black created a classification system that is widely used and based on the location of the caries on the tooth. The original classification distinguished caries into five groups, indicated by the word, "Class", and a Roman numeral. Pit and fissure caries is indicated as Class I; smooth surface caries is further divided into Class II, Class III, Class IV, and Class V. A Class VI was added onto Black's classification and also represents a smooth-surface carious lesion.
The pits and fissures of teeth provide a location for caries formation.
Pit and fissure caries
Pits and fissures are anatomic landmarks on a tooth where the enamel folds inward. Fissures are formed during the development of grooves but the enamel in the area is not fully fused. As a result, a deep linear depression forms in the enamel's surface structure, which forms a location for dental caries to develop and flourish. Fissures are mostly located on the occlusal (chewing) surfaces of posterior teeth and palatal surfaces of maxillary anterior teeth. Pits are small, pinpoint depressions that are most commonly found at the ends or cross-sections of grooves. In particular, buccal pits are found on the facial surfaces of molars. For all types of pits and fissures, the deep infolding of enamel makes oral hygiene along these surfaces difficult, allowing dental caries to develop more commonly in these areas.
The occlusal surfaces of teeth represent 12.5% of all tooth surfaces but are the location of over 50% of all dental caries. Among children, pit and fissure caries represent 90% of all dental caries. Pit and fissure caries can sometimes be difficult to detect. As the decay progresses, caries in enamel nearest the surface of the tooth spreads gradually deeper. Once the caries reaches the dentin at the dentino-enamel junction, the decay quickly spreads laterally. Within the dentin, the decay follows a triangle pattern that points to the tooth's pulp. This pattern of decay is typically described as two triangles (one triangle in enamel, and another in dentin) with their bases conjoined to each other at the dentino-enamel junction (DEJ). This base-to-base pattern is typical of pit and fissure caries, unlike smooth-surface caries (where base and apex of the two triangles join).
Smooth-surface caries
There are three types of smooth-surface caries. Proximal caries, also called interproximal caries, form on the smooth surfaces between adjacent teeth. Root caries form on the root surfaces of teeth. The third type of smooth-surface caries occur on any other smooth tooth surface.
In this radiograph, the dark spots in the adjacent teeth show proximal caries.
Proximal caries are the most difficult type to detect. Frequently, this type of caries cannot be detected visually or manually with a dental explorer. Proximal caries form cervically (toward the roots of a tooth) just under the contact between two teeth. As a result, radiographs are needed for early discovery of proximal caries. Under Black's classification system, proximal caries on posterior teeth (premolars and molars) are designated as Class II caries. Proximal caries on anterior teeth (incisors and canines) are indicated as Class III if the incisal edge (chewing surface) is not included and Class IV if the incisal edge is included.
Root caries, which are sometimes described as a category of smooth-surfaces caries, are the third most common type of caries and usually occur when the root surfaces have been exposed due to gingival recession. When the gingiva is healthy, root caries is unlikely to develop because the root surfaces are not as accessible to bacterial plaque. The root surface is more vulnerable to the demineralization process than enamel because cementum begins to demineralize at 6.7 pH, which is higher than enamel's critical pH. Regardless, it is easier to arrest the progression of root caries than enamel caries because roots have a greater reuptake of fluoride than enamel. Root caries are most likely to be found on facial surfaces, then interproximal surfaces, then lingual surfaces. Mandibular molars are the most common location to find root caries, followed by mandibular premolars, maxillary anteriors, maxillary posteriors, and mandibular anteriors.
Lesions on other smooth surfaces of teeth are also possible. Since these occur in all smooth surface areas of enamel except for interproximal areas, these types of caries are easily detected and are associated with high levels of plaque and diets promoting caries formation. Under Black's classification system, caries near the gingiva on the facial or lingual surfaces is designated Class V. Class VI is reserved for caries confined to cusp tips on posterior teeth or incisal edges of anterior teeth.
Other general descriptions
Besides the two previously mentioned categories, carious lesions can be described further by their location on a particular surface of a tooth. Caries on a tooth's surface that are nearest the cheeks or lips are called "facial caries", and caries on surfaces facing the tongue are known as "lingual caries". Facial caries can be subdivided into buccal (when found on the surfaces of posterior teeth nearest the cheeks) and labial (when found on the surfaces of anterior teeth nearest the lips). Lingual caries can also be described as palatal when found on the lingual surfaces of maxillary teeth because they are located beside the hard palate.
Caries near a tooth's cervix—the location where the crown of a tooth and its roots meet—are referred to as cervical caries. Occlusal caries are found on the chewing surfaces of posterior teeth. Incisal caries are caries found on the chewing surfaces of anterior teeth. Caries can also be described as "mesial" or "distal." Mesial signifies a location on a tooth closer to the median line of the face, which is located on a vertical axis between the eyes, down the nose, and between the contact of the central incisors. Locations on a tooth further away from the median line are described as distal.
Etiology
Rampant caries.
In some instances, caries are described in other ways that might indicate the cause. "Baby bottle caries", "early childhood caries", or "baby bottle tooth decay" is a pattern of decay found in young children with their deciduous (baby) teeth. The teeth most likely affected are the maxillary anterior teeth, but all teeth can be affected. The name for this type of caries comes from the fact that the decay usually is a result of allowing children to fall asleep with sweetened liquids in their bottles or feeding children sweetened liquids multiple times during the day. Another pattern of decay is "rampant caries", which signifies advanced or severe decay on multiple surfaces of many teeth. Rampant caries may be seen in individuals with xerostomia, poor oral hygiene, stimulant use (due to drug-induced dry mouth), and/or large sugar intake. If rampant caries is a result of previous radiation to the head and neck, it may be described as radiation-induced caries. Problems can also be caused by the self destruction of roots and whole tooth resorption when new teeth erupt or later from unknown causes.
Rate of progression
Temporal descriptions can be applied to caries to indicate the progression rate and previous history. "Acute" signifies a quickly developing condition, whereas "chronic" describes a condition which has taken an extended time to develop where thousands of meals and snacks, many causing some acid demineralisation that is not remineralised and eventually results in cavities.
Recurrent caries, also described as secondary, are caries that appears at a location with a previous history of caries. This is frequently found on the margins of fillings and other dental restorations. On the other hand, incipient caries describes decay at a location that has not experienced previous decay. Arrested caries describes a lesion on a tooth which was previously demineralized but was remineralized before causing a cavitation.
Affected hard tissue
Depending on which hard tissues are affected, it is possible to describe caries as involving enamel, dentin, or cementum. Early in its development, caries may affect only enamel. Once the extent of decay reaches the deeper layer of dentin, "dentinal caries" is used. Since cementum is the hard tissue that covers the roots of teeth, it is not often affected by decay unless the roots of teeth are exposed to the mouth. Although the term "cementum caries" may be used to describe the decay on roots of teeth, very rarely does caries affect the cementum alone. Roots have a very thin layer of cementum over a large layer of dentin, and thus most caries affecting cementum also affects dentin.
Signs and symptoms
Dental explorer used for caries diagnosis.
A person experiencing caries may not be aware of the disease. The earliest sign of a new carious lesion is the appearance of a chalky white spot on the surface of the tooth, indicating an area of demineralization of enamel. This is referred to as incipient decay. As the lesion continues to demineralize, it can turn brown but will eventually turn into a cavitation ("cavity"). Before the cavity forms, the process is reversible, but once a cavity forms, the lost tooth structure cannot be regenerated. A lesion which appears brown and shiny suggests dental caries was once present but the demineralization process has stopped, leaving a stain. A brown spot which is dull in appearance is probably a sign of active caries.
As the enamel and dentin are destroyed, the cavity becomes more noticeable. The affected areas of the tooth change color and become soft to the touch. Once the decay passes through enamel, the dentinal tubules, which have passages to the nerve of the tooth, become exposed and cause the tooth to hurt. The pain may worsen with exposure to heat, cold, or sweet foods and drinks. Dental caries can also cause bad breath and foul tastes. In highly progressed cases, infection can spread from the tooth to the surrounding soft tissues. Complications such as cavernous sinus thrombosis and Ludwig's angina can be life-threatening.
Causes
There are four main criteria required for caries formation: a tooth surface (enamel or dentin); caries-causing bacteria; fermentable carbohydrates (such as sucrose); and time. The caries process does not have an inevitable outcome, and different individuals will be susceptible to different degrees depending on the shape of their teeth, oral hygiene habits, and the buffering capacity of their saliva. Dental caries can occur on any surface of a tooth which is exposed to the oral cavity, but not the structures which are retained within the bone.
Teeth
There are certain diseases and disorders affecting teeth which may leave an individual at a greater risk for caries. Amelogenesis imperfecta, which occurs between 1 in 718 and 1 in 14,000 individuals, is a disease in which the enamel does not fully form or forms in insufficient amounts and can fall off a tooth. In both cases, teeth may be left more vulnerable to decay because the enamel is not able to protect the tooth.
In most people, disorders or diseases affecting teeth are not the primary cause of dental caries. Ninety-six percent of tooth enamel is composed of minerals. These minerals, especially hydroxyapatite, will become soluble when exposed to acidic environments. Enamel begins to demineralize at a pH of 5.5. Dentin and cementum are more susceptible to caries than enamel because they have lower mineral content. Thus, when root surfaces of teeth are exposed from gingival recession or periodontal disease, caries can develop more readily. Even in a healthy oral environment, however, the tooth is susceptible to dental caries.
The anatomy of teeth may affect the likelihood of caries formation. Where the deep grooves of teeth are more numerous and exaggerated, pit and fissure caries are more likely to develop. Also, caries are more likely to develop when food is trapped between teeth.
A gram stain image of Streptococcus mutans.
Bacteria
The mouth contains a wide variety of oral bacteria, but only a few specific species of bacteria are believed to cause dental caries: Streptococcus mutans and Lactobacilli among them. Lactobacillus acidophilus, Actinomyces viscosus, Nocardia spp., and Streptococcus mutans are most closely associated with caries, particularly root caries. Bacteria collect around the teeth and gums in a sticky, creamy-coloured mass called plaque, which serves as a biofilm. Some sites collect plaque more commonly than others. The grooves on the biting surfaces of molar and premolar teeth provide microscopic retention, as does the point of contact between teeth. Plaque may also collect along the gingiva.
Fermentable carbohydrates
Bacteria in a person's mouth convert glucose, fructose, and most commonly sucrose (table sugar) into acids such as lactic acid through a glycolytic process called fermentation. If left in contact with the tooth, these acids may cause demineralization, which is the dissolution of its mineral content. The process is dynamic, however, as remineralization can also occur if the acid is neutralized by saliva or mouthwash. Fluoride toothpaste or dental varnish may aid remineralization. If demineralization continues over time, enough mineral content may be lost so that the soft organic material left behind disintegrates, forming a cavity or hole. The impact such sugars have on the progress of dental caries is called its cariogenicity. Sucrose, although a bound glucose and fructose unit, is in fact more cariogenic than a mixture of equal parts of glucose and fructose. This is due to the bacteria utilising the energy in the saccharide bond between the glucose and fructose subunits.
Time
The frequency of which teeth are exposed to cariogenic (acidic) environments affects the likelihood of caries development. After meals or snacks, the bacteria in the mouth metabolize sugar, resulting in an acidic by-product which decreases pH. As time progresses, the pH returns to normal due to the buffering capacity of saliva and the dissolved mineral content of tooth surfaces. During every exposure to the acidic environment, portions of the inorganic mineral content at the surface of teeth dissolves and can remain dissolved for 2 hours. Since teeth are vulnerable during these acidic periods, the development of dental caries relies heavily on the frequency of acid exposure.
The carious process can begin within days of a tooth erupting into the mouth if the diet is sufficiently rich in suitable carbohydrates. Evidence suggests that the introduction of fluoride treatments have slowed the process. Proximal caries take an average of four years to pass through enamel in permanent teeth. Because the cementum enveloping the root surface is not nearly as durable as the enamel encasing the crown, root caries tends to progress much more rapidly than decay on other surfaces. The progression and loss of mineralization on the root surface is 2.5 times faster than caries in enamel. In very severe cases where oral hygiene is very poor and where the diet is very rich in fermentable carbohydrates, caries may cause cavities within months of tooth eruption. This can occur, for example, when children continuously drink sugary drinks from baby bottles.
Other risk factors
Reduced saliva is associated with increased caries since the buffering capability of saliva is not present to counterbalance the acidic environment created by certain foods. As a result, medical conditions that reduce the amount of saliva produced by salivary glands, particularly the submandibular gland and parotid gland, are likely to lead to widespread tooth decay. Examples include Sjögren's syndrome, diabetes mellitus, diabetes insipidus, and sarcoidosis. Medications, such as antihistamines and antidepressants, can also impair salivary flow. Moreover, sixty-three percent of the most commonly prescribed medications in the United States list dry mouth as a known side effect. Radiation therapy of the head and neck may also damage the cells in salivary glands, increasing the likelihood of caries formation.
The use of tobacco may also increase the risk for caries formation. Some brands of smokeless tobacco contain high sugar content, increasing susceptibility to caries. Tobacco use is a significant risk factor for periodontal disease, which can cause the gingiva to recede. As the gingiva loses attachment to the teeth, the root surface becomes more visible in the mouth. If this occurs, root caries is a concern since the cementum covering the roots of teeth is more easily demineralized by acids than enamel. Currently, there is not enough evidence to support a causal relationship between smoking and coronal caries, but evidence does suggest a relationship between smoking and root-surface caries.
Pathophysiology
The progression of pit and fissure caries resembles two triangles with their bases meeting along the junction of enamel and dentin.
Enamel
Enamel is a highly mineralized acellular tissue, and caries act upon it through a chemical process brought on by the acidic environment produced by bacteria. As the bacteria consume the sugar and use it for their own energy, they produce lactic acid. The effects of this process include the demineralization of crystals in the enamel, caused by acids, over time until the bacteria physically penetrate the dentin. Enamel rods, which are the basic unit of the enamel structure, run perpendicularly from the surface of the tooth to the dentin. Since demineralization of enamel by caries generally follows the direction of the enamel rods, the different triangular patterns between pit and fissure and smooth-surface caries develop in the enamel because the orientation of enamel rods are different in the two areas of the tooth .
As the enamel loses minerals , and dental caries progress, they develop several distinct zones, visible under a light microscope. From the deepest layer of the enamel to the enamel surface, the identified areas are the: translucent zone, dark zones, body of the lesion, and surface zone. The translucent zone is the first visible sign of caries and coincides with a 1-2% loss of minerals. A slight remineralization of enamel occurs in the dark zone, which serves as an example of how the development of dental caries is an active process with alternating changes. The area of greatest demineralization and destruction is in the body of the lesion itself. The surface zone remains relatively mineralized and is present until the loss of tooth structure results in a cavitation.
Dentin
Unlike enamel, the dentin reacts to the progression of dental caries. After tooth formation, the ameloblasts, which produce enamel, are destroyed once enamel formation is complete and thus cannot later regenerate enamel after its destruction. On the other hand, dentin is produced continuously throughout life by odontoblasts, which reside at the border between the pulp and dentin. Since odontoblasts are present, a stimulus, such as caries, can trigger a biologic response. These defense mechanisms include the formation of sclerotic and tertiary dentin.
In dentin from the deepest layer to the enamel, the distinct areas affected by caries are the translucent zone, the zone of bacterial penetration, and the zone of destruction. The translucent zone represents the advancing front of the carious process and is where the initial demineralization begins. The zones of bacterial penetration and destruction are the locations of invading bacteria and ultimately the decomposition of dentin.
The faster spread of caries through dentin creates this triangular appearance in smooth surface caries.
Sclerotic dentin
The structure of dentin is an arrangement of microscopic channels, called dentinal tubules, which radiate outward from the pulp chamber to the exterior cementum or enamel border. The diameter of the dentinal tubules is largest near the pulp (about 2.5 μm) and smallest (about 900 nm) at the junction of dentin and enamel. The carious process continues through the dentinal tubules, which are responsible for the triangular patterns resulting from the progression of caries deep into the tooth. The tubules also allow caries to progress faster.
In response, the fluid inside the tubules bring immunoglobulins from the immune system to fight the bacterial infection. At the same time, there is an increase of mineralization of the surrounding tubules. This results in a constriction of the tubules, which is an attempt to slow the bacterial progression. In addition, as the acid from the bacteria demineralizes the hydroxyapatite crystals, calcium and phosphorus are released, allowing for the precipitation of more crystals which fall deeper into the dentinal tubule. These crystals form a barrier and slow the advancement of caries. After these protective responses, the dentin is considered sclerotic.
Fluids within dentinal tubules are believed to be the mechanism by which pain receptors are triggered within the pulp of the tooth. Since sclerotic dentin prevents the passage of such fluids, pain that would otherwise serve as a warning of the invading bacteria may not develop at first. Consequently, dental caries may progress for a long period of time without any sensitivity of the tooth, allowing for greater loss of tooth structure.
Tertiary dentin
In response to dental caries, there may the production of more dentin toward the direction of the pulp. This new dentin is referred to as tertiary dentin. Tertiary dentin is produced to protect the pulp for as long as possible from the advancing bacteria. As more tertiary dentin is produced, the size of the pulp decreases. This type of dentin has been subdivided according to the presence or absence of the original odontoblasts. If the odontoblasts survive long enough to react to the dental caries, then the dentin produced is called "reactionary" dentin. If the odontoblasts are killed, the dentin produced is called "reparative" dentin.
In the case of reparative dentin, other cells are needed to assume the role of the destroyed odontoblasts. Growth factors, especially TGF-β, are thought to initiate the production of reparative dentin by fibroblasts and mesenchymal cells of the pulp. Reparative dentin is produced at an average of 1.5 μm/day, but can be increased to 3.5 μm/day. The resulting dentin contains irregularly-shaped dentinal tubules which may not line up with existing dentinal tubules. This diminishes the ability for dental caries to progress within the dentinal tubules.
Diagnosis
(A) A small spot of decay visible on the surface of a tooth. (B) The radiograph reveals an extensive region of demineralization within the dentin (arrows). (C) A hole is discovered on the side of the tooth at the beginning of decay removal. (D) All decay removed.
Primary diagnosis involves inspection of all visible tooth surfaces using a good light source, dental mirror and explorer. Dental radiographs (X-rays) may show dental caries before it is otherwise visible, particularly caries between the teeth. Large dental caries are often apparent to the naked eye, but smaller lesions can be difficult to identify. Visual and tactile inspection along with radiographs are employed frequently among dentists, particularly to diagnose pit and fissure caries. Early, uncavitated caries is often diagnosed by blowing air across the suspect surface, which removes moisture and changes the optical properties of the unmineralized enamel.
Some dental researchers have cautioned against the use of dental explorers to find caries. In cases where a small area of tooth has begun demineralizing but has not yet cavitated, the pressure from the dental explorer could cause a cavity. Since the carious process is reversible before a cavity is present, it may be possible to arrest the caries with fluoride and remineralize the tooth surface. When a cavity is present, a restoration will be needed to replace the lost tooth structure.
At times, pit and fissure caries may be difficult to detect. Bacteria can penetrate the enamel to reach dentin, but then the outer surface may remineralize, especially if fluoride is present. These caries, sometimes referred to as "hidden caries", will still be visible on x-ray radiographs, but visual examination of the tooth would show the enamel intact or minimally perforated.
Treatment
An amalgam used as a restorative material in a tooth.
Destroyed tooth structure does not fully regenerate, although remineralization of very small carious lesions may occur if dental hygiene is kept at optimal level. For the small lesions, topical fluoride is sometimes used to encourage remineralization. For larger lesions, the progression of dental caries can be stopped by treatment. The goal of treatment is to preserve tooth structures and prevent further destruction of the tooth.
Generally, early treatment is less painful and less expensive than treatment of extensive decay. Anesthetics — local, nitrous oxide ("laughing gas"), or other prescription medications — may be required in some cases to relieve pain during or following treatment or to relieve anxiety during treatment. A dental handpiece ("drill") is used to remove large portions of decayed material from a tooth. A spoon is a dental instrument used to remove decay carefully and is sometimes employed when the decay in dentin reaches near the pulp. Once the decay is removed, the missing tooth structure requires a dental restoration of some sort to return the tooth to functionality and aesthetic condition.
Restorative materials include dental amalgam, composite resin, porcelain, and gold. Composite resin and porcelain can be made to match the color of a patient's natural teeth and are thus used more frequently when aesthetics are a concern. Composite restorations are not as strong as dental amalgam and gold; some dentists consider the latter as the only advisable restoration for posterior areas where chewing forces are great. When the decay is too extensive, there may not be enough tooth structure remaining to allow a restorative material to be placed within the tooth. Thus, a crown may be needed. This restoration appears similar to a cap and is fitted over the remainder of the natural crown of the tooth. Crowns are often made of gold, porcelain, or porcelain fused to metal.
A tooth with extensive caries eventually requiring extraction.
In certain cases, endodontic therapy may be necessary for the restoration of a tooth. Endodontic therapy, also known as a "root canal", is recommended if the pulp in a tooth dies from infection by decay-causing bacteria or from trauma. During a root canal, the pulp of the tooth, including the nerve and vascular tissues, is removed along with decayed portions of the tooth. The canals are instrumented with endodontic files to clean and shape them, and they are then usually filled with a rubber-like material called gutta percha. The tooth is filled and a crown can be placed. Upon completion of a root canal, the tooth is now non-vital, as it is devoid of any living tissue.
An extraction can also serve as treatment for dental caries. The removal of the decayed tooth is performed if the tooth is too far destroyed from the decay process to effectively restore the tooth. Extractions are sometimes considered if the tooth lacks an opposing tooth or will probably cause further problems in the future, as may be the case for wisdom teeth. Extractions may also be preferred by patients unable or unwilling to undergo the expense or difficulties in restoring the tooth.
Prevention
Toothbrushes are commonly used to clean teeth.
Oral hygiene
Personal hygiene care consists of proper brushing and flossing daily. The purpose of oral hygiene is to minimize any etiologic agents of disease in the mouth. The primary focus of brushing and flossing is to remove and prevent the formation of plaque. Plaque consists mostly of bacteria. As the amount of bacterial plaque increases, the tooth is more vulnerable to dental caries when carbohydrates in the food are left on teeth after every meal or snack. A toothbrush can be used to remove plaque on accessible surfaces, but not between teeth or inside pits and fissures on chewing surfaces. When used correctly, dental floss removes plaque from areas which could otherwise develop proximal caries. Other adjunct hygiene aids include interdental brushes, water picks, and mouthwashes.
However oral hygiene is probably more effective at preventing gum disease than tooth decay. The brush and fluoride toothpaste have no access inside pits and fissures, where chewing forces food to be trapped. It is here that resident plaque bacteria change any carbohydrate to acid that demineralises teeth inside pits and fissures, causing over 80% of cavities. (Occlusal caries accounts for between 80 and 90 percent of caries in children (Weintraub, 2001). The teeth at highest risk for carious lesions are the first and second permanent molars.)
Chewing fibre like celery after eating forces saliva inside pits and fissures to dilute any carbohydrate like sugar in trapped food, neutralise acid and remineralise demineralised tooth and should be part of every day personal tooth care to prevent tooth decay.
Professional hygiene care consists of regular dental examinations and cleanings. Sometimes, complete plaque removal is difficult, and a dentist or dental hygienist may be needed. Along with oral hygiene, radiographs may be taken at dental visits to detect possible dental caries development in high risk areas of the mouth.
Dietary modification
For dental health, frequency of sugar intake is more important than the amount of sugar consumed. In the presence of sugar and other carbohydrates, bacteria in the mouth produce acids which can demineralize enamel, dentin, and cementum. The more frequently teeth are exposed to this environment, the more likely dental caries are to occur. Therefore, minimizing snacking is recommended, since snacking creates a continual supply of nutrition for acid-creating bacteria in the mouth. Also, chewy and sticky foods (such as dried fruit or candy) tend to adhere to teeth longer, and consequently are best eaten as part of a meal. Brushing the teeth after meals is recommended. For children, the American Dental Association and the European Academy of Paediatric Dentistry recommend limiting the frequency of consumption of drinks with sugar, and not giving baby bottles to infants during sleep. Mothers are also recommended to avoid sharing utensils and cups with their infants to prevent transferring bacteria from the mother's mouth.
It has been found that milk and certain kinds of cheese like cheddar can help counter tooth decay if eaten soon after the consumption of foods potentially harmful to teeth. Also, chewing gum containing xylitol (a sugar alcohol) is widely used to protect teeth in some countries, being especially popular in the Finnish candy industry. Xylitol's effect on reducing plaque is probably due to bacteria's inability to utilize it like other sugars. Chewing and stimulation of flavour receptors on the tongue are also known to increase the production and release of saliva, which contains natural buffers to prevent the lowering of pH in the mouth to the point where enamel may become demineralised.
Common dentistry trays used to deliver fluoride.
Other preventive measures
The use of dental sealants is a means of prevention. A sealant is a thin plastic-like coating applied to the chewing surfaces of the molars. This coating prevents food being trapped inside pits and fissures in grooves under chewing pressure so resident plaque bacteria are deprived of carbohydrate that they change to acid demineralisation and thus prevents the formation of pit and fissure caries, the most common form of dental caries. Sealants are usually applied on the teeth of children, shortly after the molars erupt. Older people may also benefit from the use of tooth sealants, but their dental history and likelihood of caries formation are usually taken into consideration.
Calcium, as found in milk and green vegetables are often recommended to protect against dental caries. It has been demonstrated that Calcium and fluoride supplements decrease the incidence of dental caries. Fluoride helps prevent decay of a tooth by binding to the hydroxyapatite crystals in enamel. The incorporated Calcium makes enamel more resistant to demineralization and, thus, resistant to decay. Topical fluoride is also recommended to protect the surface of the teeth. This may include a fluoride toothpaste or mouthwash. Many dentists include application of topical fluoride solutions as part of routine visits.
Furthermore, recent research shows that low intensity laser radiation of argon ion lasers may prevent the susceptibility for enamel caries and white spot lesions. Also, as bacteria are a major factor contributing to poor oral health, there is currently research to find a vaccine for dental caries. As of 2004, such a vaccine has been successfully tested on animals, and is in clinical trials for humans as of May 2006.
Epidemiology
Worldwide, most children and an estimated ninety percent of adults have experienced caries, with the disease most prevalent in Asian and Latin American countries and least prevalent in African countries. In the United States, dental caries is the most common chronic childhood disease, being at least five times more common than asthma. It is the primary pathological cause of tooth loss in children. Between 29% and 59% of adults over the age of fifty experience caries.
The number of cases has decreased in some developed countries, and this decline is usually attributed to increasingly better oral hygiene practices and preventive measures such as fluoride treatment. Nonetheless, countries that have experienced an overall decrease in cases of tooth decay continue to have a disparity in the distribution of the disease. Among children in the United States and Europe, twenty percent of the population endures sixty to eighty percent of cases of dental caries. A similarly skewed distribution of the disease is found throughout the world with some children having none or very few caries and others having a high number. Australia, Nepal, and Sweden have a low incidence of cases of dental caries among children, whereas cases are more numerous in Costa Rica and Slovakia.
The classic "DMF" (decay/missing/filled) index is one of the most common methods for assessing caries prevalence as well as dental treatment needs among populations. This index is based on in-field clinical examination of individuals by using a probe, mirror and cotton rolls. Because the DMF index is done without X-ray imaging, it underestimates real caries prevalence and treatment needs.
History
An image from 1300s (A.D.) England depicting a dentist extracting a tooth with forceps.
There is a long history of dental caries. Over a million years ago, hominids such as Australopithecus suffered from cavities. The largest increases in the prevalence of caries have been associated with dietary changes. Archaeological evidence shows that tooth decay is an ancient disease dating far into prehistory. Skulls dating from a million years ago through the neolithic period show signs of caries, excepting those from the Paleolithic and Mesolithic ages. The increase of caries during the neolithic period may be attributed to the increase of plant foods containing carbohydrates. The beginning of rice cultivation in South Asia is also believed to have caused an increase in caries.
A Sumerian text from 5000 BC describes a "tooth worm" as the cause of caries. Evidence of this belief has also been found in India, Egypt, Japan, and China.
Unearthed ancient skulls show evidence of primitive dental work. In Pakistan, teeth dating from around 5500 BC to 7000 BC show nearly perfect holes from primitive dental drills. The Ebers Papyrus, an Egyptian text from 1550 BC, mentions diseases of teeth. During the Sargonid dynasty of Assyria during 668 to 626 BC, writings from the king's physician specify the need to extract a tooth due to spreading inflammation. In the Roman Empire, wider consumption of cooked foods led to a small increase in caries prevalence. The Greco-Roman civilization, in addition to the Egyptian, had treatments for pain resulting from caries.
The rate of caries remained low through the Bronze and Iron ages, but sharply increased during the Medieval period. Periodic increases in caries prevalence had been small in comparison to the 1000 AD increase, when sugar cane became more accessible to the Western world. Treatment consisted mainly of herbal remedies and charms, but sometimes also included bloodletting. The barber surgeons of the time provided services that included tooth extractions. Learning their training from apprenticeships, these health providers were quite successful in ending tooth pain and likely prevented systemic spread of infections in many cases. Among Roman Catholics, prayers to Saint Apollonia, the patroness of dentistry, were meant to heal pain derived from tooth infection.
There is also evidence of caries increase in North American Indians after contact with colonizing Europeans. Before colonization, North American Indians subsisted on hunter-gatherer diets, but afterwards there was a greater reliance on maize agriculture, which made these groups more susceptible to caries.
In the medieval Islamic world, Muslim physicians such as al-Gazzar and Avicenna (in The Canon of Medicine) provided the earliest known treatments for caries, though they also believed that it was caused by tooth worms as the ancients had. This was eventually proven false in 1200 by another Muslim dentist named Gaubari, who in his Book of the Elite concerning the unmasking of mysteries and tearing of veils, was the first to reject the idea of caries being caused by tooth worms, and he stated that tooth worms in fact do not even exist. The theory of the tooth worm was thus no longer accepted in the Islamic medical community from the 13th century onwards.
During the European Age of Enlightenment, the belief that a "tooth worm" caused caries was also no longer accepted in the European medical community. Pierre Fauchard, known as the father of modern dentistry, was one of the first to reject the idea that worms caused tooth decay and noted that sugar was detrimental to the teeth and gingiva. In 1850, another sharp increase in the prevalence of caries occurred and is believed to be a result of widespread diet changes. Prior to this time, cervical caries was the most frequent type of caries, but increased availability of sugar cane, refined flour, bread, and sweetened tea corresponded with a greater number of pit and fissure caries.
In the 1890s, W.D. Miller conducted a series of studies that led him to propose an explanation for dental caries that was influential for current theories. He found that bacteria inhabited the mouth and that they produced acids which dissolved tooth structures when in the presence of fermentable carbohydrates. This explanation is known as the chemoparasitic caries theory. Miller's contribution, along with the research on plaque by G.V. Black and J.L. Williams, served as the foundation for the current explanation of the etiology of caries. Several of the specific strains of bacteria were identified in 1921 by Fernando E. Rodriguez Vargas.